7. Topical Trends
This chapter highlights key trends shaping the work of family physicians and the environments in which they practice. Using multiple ABFM data sources, it examines changes in patient panel sizes, scope of care, practice organization, rural participation, educational debt, and emerging payment models. Together, these patterns illustrate how the practice of family medicine is evolving and how those changes affect access to primary care for patients and communities.
Family Physician Panel Sizes Are Shrinking
Commentary
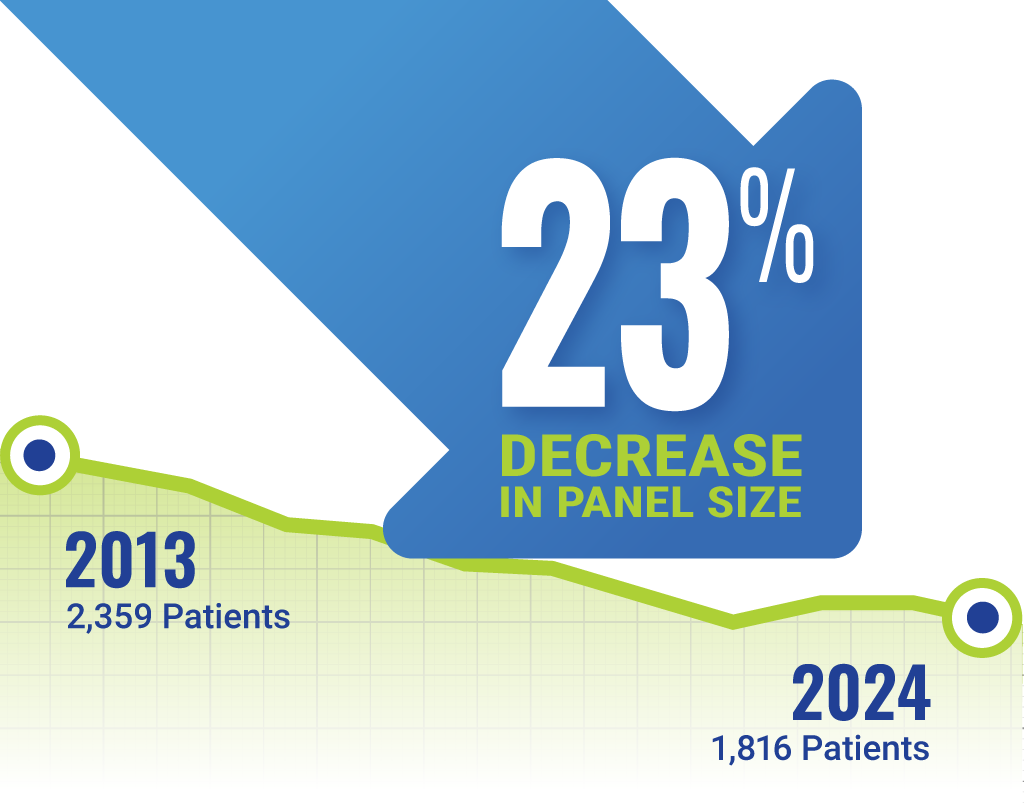
Between 2013 and 2024, average patient panel sizes decreased by 23%. This decrease likely reflects increasing complexity of patient care and growing administrative demands, which limit how many patients each primary care physician can effectively manage.
Figure 1: Family Physician Panel Size is Shrinking
Illustration: Copyright 2025 American Board of Family Medicine Source: ABFM; Population: mid-to-late career; Scope: outpatient continuity care • Get the data • Download the image

Connections and Context
Average patient panel sizes among U.S. family physicians have been declining since 2013 (Bazemore et al, 2024) with some variation according to practice, scope, and team characteristics ( Bazemore et al, 2026), even after adjusting for trends in part time work. There isn’t clear evidence on optimal panel size (Shekelle et al, 2019, Katerndahl et al, 2015), but these declines merit policymaker attention, given implications for workforce planning and access to primary care. Reversing this trajectory will require a two-pronged strategy: 1) strengthening team-based infrastructure that enables family physicians to maintain high quality primary care for larger panels through expanded team-based staffing, data support, and technology, and 2) substantially increasing the overall supply of family physicians. Without such action, declining panel size risks eroding population-level access to continuous, relationship-based primary care (Britz et al, 2025).
The Changing Scope of Care among Family Physicians
Commentary
Family physicians continue to offer a broad scope of care, but the mix of services has shifted over the last decade as increasingly complex individual outpatient care has replaced some previous models. Self-reported provision of adult inpatient medicine and obstetric care has declined significantly in both early- and mid- late-career cohorts, with mid- to late-career physicians reporting lower participation overall. Outpatient care remains central to most practices.
Connections and Context
Increasing complexity of patients and outpatient care, paired with payment shifts, administrative barriers to maintaining hospital privileges, and increasing specialization of hospital and maternity care services likely explain these declines in both inpatient and obstetric care among family physicians (Carek et al, 2024). No single factor reliably predicts family physician scope (Lambert et al, 2025). Preserving comprehensive scope does remain essential to sustaining access in underserved and rural communities, and has been clearly associated with preserving the salutary benefits of primary care (Starfield et al, 2005, Bazemore et al, 2015), an issue worthy of continued policymaker and educator conversation (Henry et al, 2022).
Declines in Practice Ownership Among Family Physicians
Commentary
Practice ownership among family physicians has declined modestly from 2016-2024. Fewer mid-to-late career physicians report sole or partial ownership, while employed arrangements, such as hospital- or system-based practices, have increased.
Figure 3: Practice Ownership in Mid- to Late-Career Family Physicians
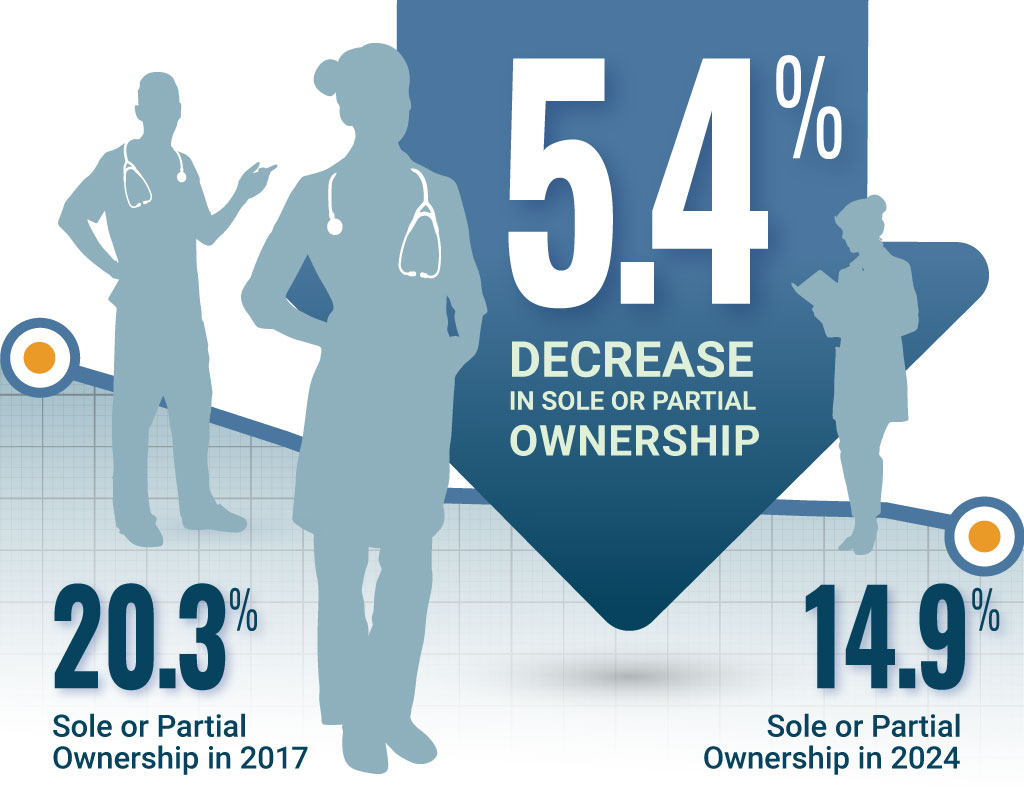

Illustration: Copyright 2025 American Board of Family Medicine Source: ABFM; Population: mid-to-late career; Scope: direct patient care • Get the data • Download the image
Connections and Context
This shift reflects broader consolidation trends in U.S. health care. While employment may offer stability and infrastructure support, it also reduces autonomy and may affect physician satisfaction and decision-making authority (Rittenhouse et al, 2021). The balance between independence and system integration continues to shape the practice landscape, with recent evidence highlighting exceptional independent family physician service despite consolidation in urban areas (Rittenhouse et al, 2024).
Outpatient Continuity Care Stable as a Principal Professional Activity
Commentary
Most family physicians report outpatient continuity care as their primary professional activity, with rates remaining high and stable through 2024. Early-career physicians increasingly align their work with longitudinal patient relationships rather than episodic or urgent care roles.
Connections and Context
Continuity is central to the identity and effectiveness of family medicine. After previously documented increases, these findings indicate that the number of family physicians who primarily provide emergency, urgent, or hospitalist care remains small and is not growing—though these clinicians continue to play a critical role in rural settings (Peterson et al, 2019). These findings reaffirm that, even amid structural and payment challenges, continuity-based care remains a defining feature of the specialty—critical to patient trust, quality outcomes, and cost efficiency.
Rural Practice Trends Among Family Physicians
Commentary
Rural practice continues to represent a substantial share of family medicine. Family medicine remains the only physician specialty with a significant rural presence, with its distribution roughly mirroring rural population patterns in the United States. Between 2016 and 2024, approximately one in six family physicians practiced in a rural area, with only small fluctuations over time.
Connections and Context
Family physicians remain the cornerstone of rural healthcare delivery. However, stagnant rural participation signals persistent recruitment and retention challenges. Sustained investment in rural training tracks, telehealth, and payment equity is vital to maintain access for rural populations (Meyers et al, 2020).
Educational Debt Trends in Family Medicine Resident Physicians
Commentary
Educational debt among family medicine residents around the time of graduation increased from approximately $205,000 to $235,000, between 2017 and 2022, before declining to $220,000 by 2024. Broader inflation since 2017 has reduced physician purchasing power, meaning that modest increases in early-career income may not offset rising costs of living and training.
Connections and Context
Educational debt has long proven a barrier to entering primary care and family medicine (Phillips et al, 2014; Phillips et al, 2021). This has significant implications for efforts to address primary care shortages and to sustain care in public and safety‑net clinics serving vulnerable populations; an especially urgent concern amid the ongoing primary care access crisis and a rapidly growing geriatric population (Phillips et al, 2019). Emerging evidence further links debt with heavier workloads and likelihood of burnout symptoms among early career family physicians (Seehusen et al, 2025). These findings underscore the need for system‑ and employer‑level strategies to reduce educational debt for physicians entering primary care in order to ensure a healthy, adequate, and sustainable physician workforce.
Family Physicians and Direct Primary Care Payments
Commentary
Direct Primary Care (DPC) is a practice model in which patients pay a recurring membership fee directly to a primary care physician for a defined set of services, typically without billing insurance for routine care. From 2017–2024, approximately 6% of family physicians providing outpatient continuity care self-report practicing in a DPC model, with only modest growth since the COVID-19 pandemic. These estimates should be interpreted cautiously: in the absence of an agreed-upon typology, self-reported DPC likely reflects a heterogeneous set of practice arrangements; the independent nature of these practices complicates tracking clinics and patients served.
Connections and Context
Clinicians entering DPC models in the last 15 years have reported improved patient relationships, longer visit times, and reduced administrative burden, but noted concerns about financial risk, limited scalability, and uncertainty about access for vulnerable populations (Eskew et al, 2015). Nonetheless, DPC is positioned to grow substantially over the next decade given Medicare regulatory changes and growing interest among clinicians; other recent estimates suggest this growth is already underway (Zhu et al, 2025).
Taken together, these trends show that family physicians are caring for patients in an environment that is becoming more complex, even as the time and capacity available for each patient is increasingly constrained. For patients, this affects how easily they can find and maintain a long-term relationship with a trusted primary care doctor who knows them and can coordinate their care across settings. For the workforce, the data highlight why sustaining access to high-quality primary care requires investment in team-based care, supportive practice structures, and policies that recognize the depth of work family physicians do. For family physicians themselves, these patterns reflect both the value of comprehensive, relationship-based care and the growing need for systems that make this work sustainable over time.
The term family physicians as used above refers to ABFM board-certified family physicians (Diplomates) and datasets related to ABFM proprietary surveys.
