On this page
4. How Are Family Medicine Practices Organized and Structured?
Family physicians who reported practicing outpatient continuity care were surveyed on further questions pertaining to their practice organization and structure.
Practice Sites
The plurality of American Board of Family Medicine (ABFM) Diplomates report a principal practice site at a hospital- or health-system owned medical practice (35.3%) or at an independently-owned practice (30.7%). A greater percentage of mid-or late career Diplomates reported working in independently-owned practices compared to early career physicians (30.7% vs. 14.0%). On the other hand, a higher proportion of early career Diplomates reported working in Federally-Qualified Health Centers (12.3% vs. 6.7%) and academic health centers (11.8% vs. 7.6%) compared to the majority of Diplomates.
Less than half of family physicians (43.5%) report practicing in multiple sites. The most common setting for a secondary site was at a hospital (20.9%). When comparing early career Diplomates with mid-or late career Diplomates, a greater percentage reported secondary practice sites in another outpatient clinic (11.6% v. 5.7%), urgent care clinic (12.4% vs. 7.9%), or emergency department (6.3% v. 4.4%). Interestingly, a lower percentage of early career respondents reported a secondary site of a nursing home or assisted living facility (11.9% vs. 13.4%). See Chapter 7 for more detailed facts on scope of practice.
TABLE 3. Reported Practice Sites by Family Physicians
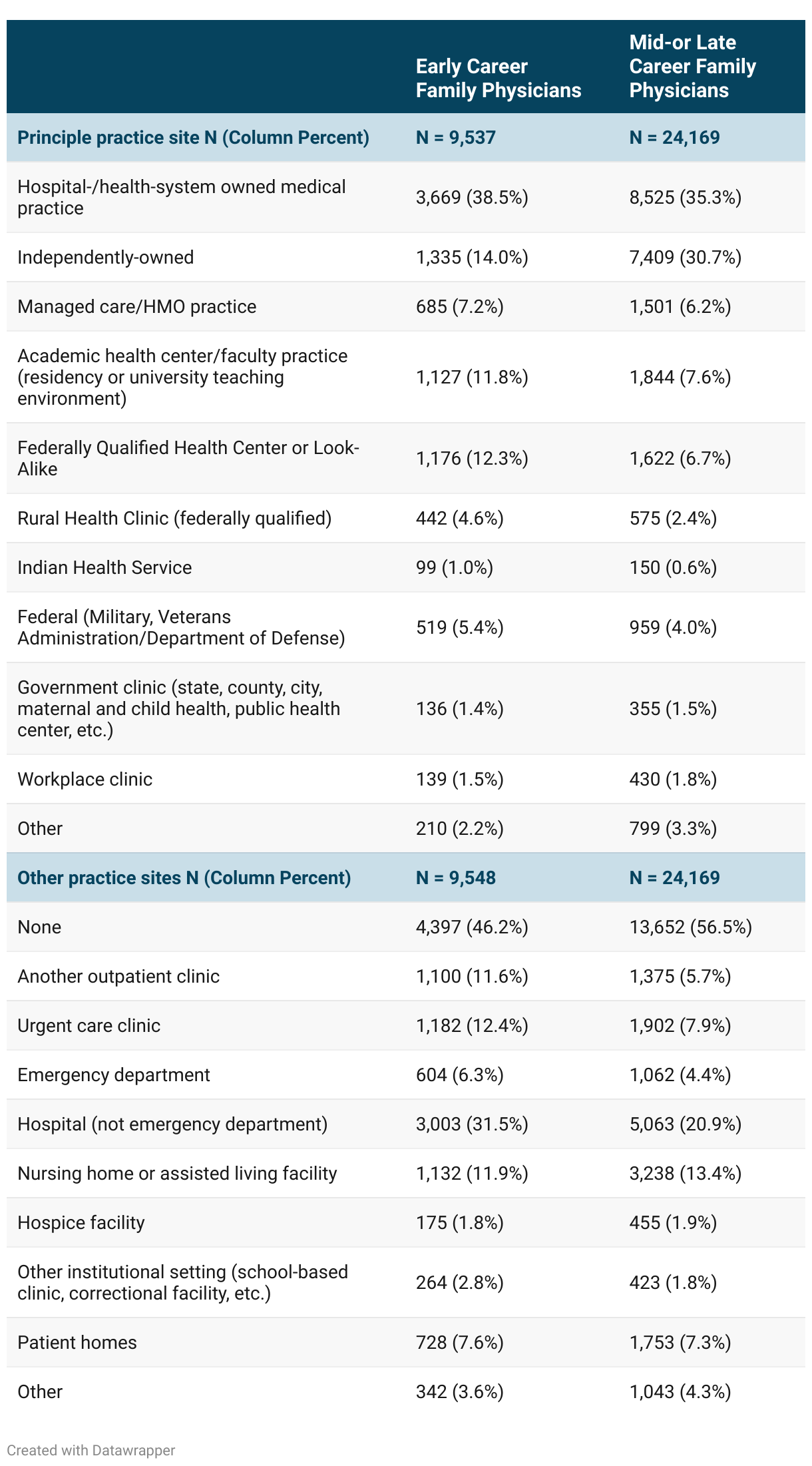
FIGURE 11: Family Physicians by Practice Site

FIGURE 12: Comparison of Early and Mid-or Late Career Family Physicians by Practice Site

Practice Site Characteristics
Family physicians were asked to provide further information about their primary practice sites to characterize ownership status, practice size, and specialty mix. The majority did not have an official ownership stake in their practice sites. Family medicine practices also tend to have more than one provider (89.5%), and the plurality of Diplomates work in practices that only have family medicine providers (50.3%). ABFM Diplomates early in their careers were much less likely to have an ownership stake or work in solo practice compared to the greater majority of Diplomates.
TABLE 4. Reported Practice Characteristics by Family Physicians

FIGURE 13: Comparison of Early and Mid-or Late Career Family Physicians by Practice Ownership

FIGURE 14. Comparison of Early and Mid-or Late Career Family Physicians by Practice Size and Specialty Mix

Practice Payment
Family medicine physicians are predominantly reimbursed by payers through a fee-for-service (FFS) model, through which practices bill for delivering specific services, collect copays from patients, and are reimbursed by payers based on services provided. This model not only incentivizes increased service volume, but also limits flexibility in care planning and makes health care feel transactional.18 Alternative payment models, redefining quality measures, and increasing investments in primary care are ongoing initiatives supported by ABFM to address issues in health care payment models.19-21 As decision makers evaluate and debate payment reform, it is important to understand the payor groups that contribute to family medicine practices. ABFM Diplomates were asked to identify payers that make up the majority of their primary practice site revenue. The most common payers identified were Medicare (86.1%) and commercial insurance (85.6%), followed by direct payment (self-pay, 77.4%) and Medicaid / the Children’s Health Insurance Program (CHIP) (70.0%).
TABLE 5: Reported Payers Contributing to Revenue at Family Practices

FIGURE 15. Payers Contributing to Revenue at Family Practices

Practice Population Characteristics
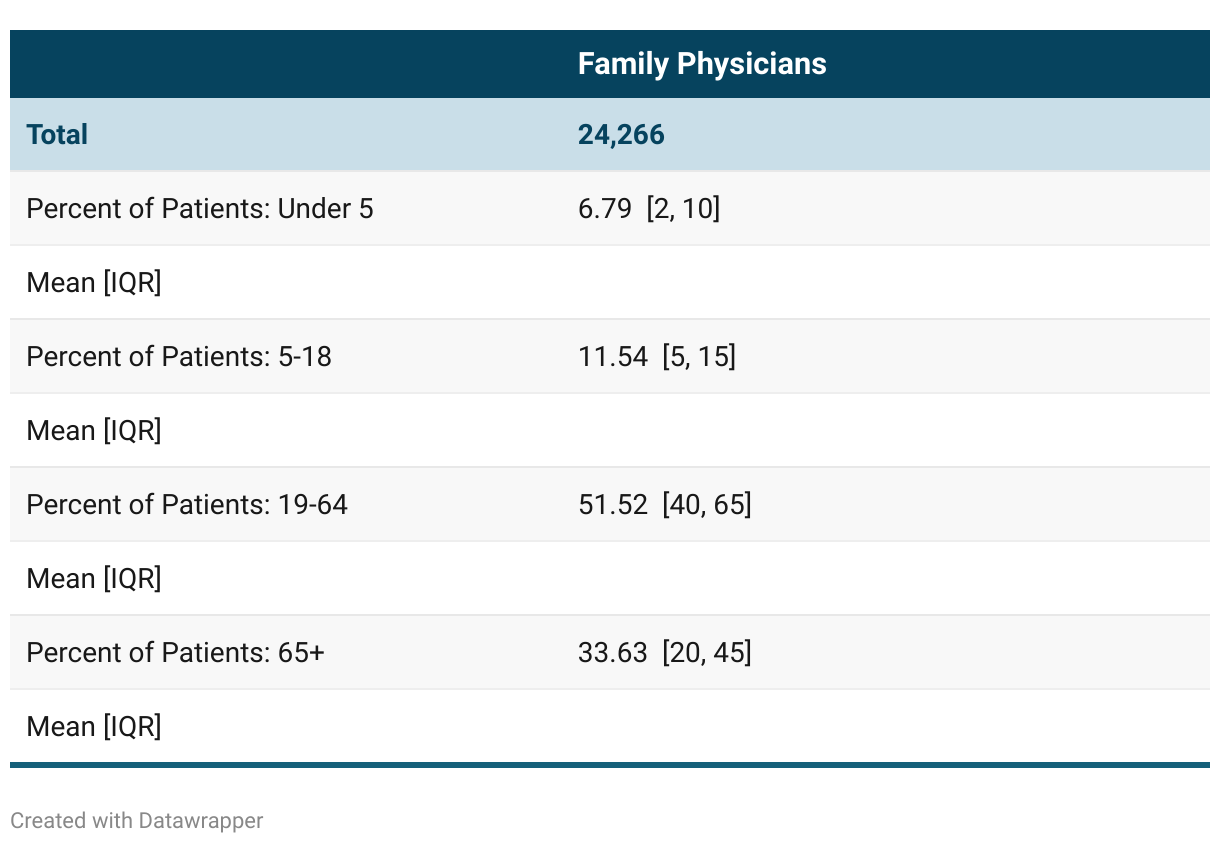
Family physicians were asked to estimate the percentage of patients they saw across specific age ranges with total sum to 100%: age <5, age 5-18, age 19-64, and age 65+. While this data is limited by self-reporting, average values revealed that approximately 85% of patients in Diplomate patient panels are in the adult range (19+).
TABLE 6. Population Ages Reported at Family Practices
Compared to other primary care physicians, family physicians care for a greater proportion of historically underserved patient groups.22 Physicians surveyed were asked to estimate the proportion of their patients that were part of a historically marginalized group, defined as “uninsured, covered by Medicaid insurance, homeless, low income, non-English speaking, racial/ethnic minority, or otherwise traditionally underserved”. Approximately one in five Diplomates reported that over half of their patients were a part of such a group.
TABLE 7. Proportion of Vulnerable Patients Reported at Family Practices

Patient-Centered Medical Home
The patient-centered medical home (PCMH) model was launched in 2007 to promote comprehensive primary care. To be formally designated as a PCMH, primary care practices undergo an accreditation process through a state or national organization that has specific requirements determined by the organization. The National Committee for Quality Assurance (NCQA) is the most widely adopted PCMH model for practices in the U.S.26 Among ABFM Diplomates who work in outpatient continuity care, 42.2% report working at a recognized PCMH.
TABLE 8. Patient-Centered Medical Home Status of Family Practices

